Resuming Normal Practice: Malaria and COVID-19
Open article published on MedShr: 9th December 2020
Last updated: 9th December 2020
Every effort has been made to ensure that the information contained in this article is accurate and current at time of publication, but if you notice an error please contact covid@medshr.net and we will aim to address this. Please find MedShr’s full terms of service here.
Malaria and COVID-19
On 30th November, the World Health Organization (WHO) published the World Malaria Report 2020, with a special section highlighting the impact of the COVID-19 pandemic on the global response to malaria.[1]
All malaria endemic countries had reported cases of SARS-CoV-2 virus by April 2020.[1] Early in the pandemic, authors and organisations around the world called for urgent actions to ensure that the global pandemic does not lead to a dramatic reversal of the progress made in managing malaria over the past two decades.[1, 2, 3] It was feared that in low- and middle-income countries (LIMCs) where there is already a considerable burden of communicable disease, increased pressure on healthcare systems combined with disruption to health promotion programmes may lead to substantial indirect excess morbidity and mortality associated with COVID-19.[2]
Modelling analysis performed by the malaria cross-partner effort for COVID-19, convened in March 2020 by the WHO, examined the potential excess morbidity and mortality from malaria in sub-Saharan Africa during 2020 in a range of scenarios where access to effective antimalarial treatment and/or insecticide treated nets was reduced by the pandemic.[4] In the most severe scenario, where a 75% reduction in access to both insecticide-treated nets (ITNs) and effective antimalarial treatment occurs, with no ITN prevention campaigns in those countries who had planned campaigns, the mortality from malaria in sub-Saharan Africa could be 100% higher than in 2018 (an estimated 769,000 malaria deaths).[4] The potentially devastating impact highlighted by this analysis led to calls for global action and the production of the WHO World Malaria Project guidance, ‘Tailoring malaria interventions in the COVID-19 response’.[5]
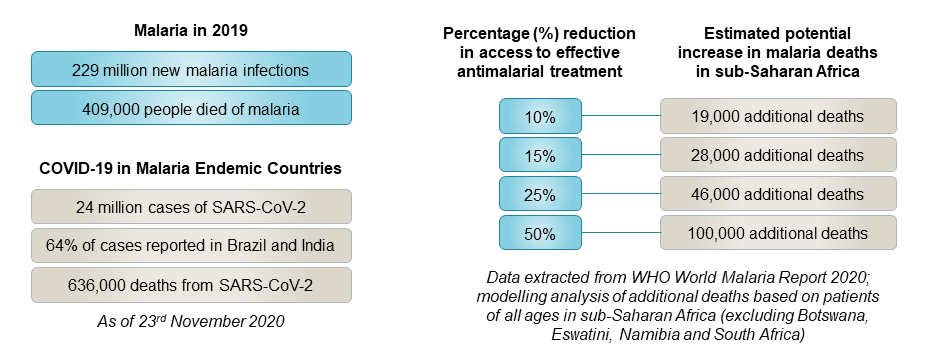
Positively, the most recent data presented in the World Malaria Report 2020 predicts that most countries in sub-Saharan Africa will complete preventative programmes as planned this year despite some initial delays. However, the analysis in the report highlights that even moderate levels of disruption in access to effective antimalarials could still lead to marked increases in malaria deaths, even if all prevention campaigns for insecticide treated nets are completed (see figue 1).[1]
Challenges for Malaria Prevention and Treatment During the COVID-19 Pandemic
Examining the effects of the recent Ebola virus disease outbreak in west Africa demonstrates the indirect impact disease outbreaks can have on other communicable diseases, such as malaria.[5, 6, 7]
Analysis suggests that as malaria and Ebola virus disease share common clinical features (especially fever), this had a marked impact on care-seeking behaviours and led to difficulties in making an early diagnosis; in a similar way, COVID-19 and malaria also share common clinical features.[5] Additionally, further disruption to malaria prevention and management programmes resulted from decreased healthcare capacity as services are adapted to manage the disease outbreak and public health mitigation strategies are implemented.[7]
Based on the World Malaria Report 2020, and other available literature, some potential challenges for maintaining essential malaria services during the COVID-19 pandemic include:
Diagnostic challenge: Although data suggests severe, symptomatic SARS-CoV-2 infection in young children is less common than in older adults [8] - a trend which is opposite to the burden of infection from malaria where children under 5 are most vulnerable - both infections share common presenting symptoms, predominantly fever.[5, 9] This presents a diagnostic challenge, particularly in settings where access to rapid diagnostic testing may be limited.[9] In their perspective article, Aborode et al. [10] highlight the importance of considering both infections in patients presenting with fever.
Communication and public health messaging: In the early stages of the pandemic in particular, public health messaging advised staying at home if you developed a fever to try and reduce the transmission of SARS-CoV-2, but this may have reduced the number of patients presenting with febrile illness due to malaria.[1] As untreated cases of malaria can rapidly progress to severe infection and death, the WHO has highlighted the importance of adapting public health messaging in malaria endemic settings to encourage seeking immediate treatment for fever.[11]
Effects on the healthcare workforce: healthcare workers who normally provide services to help prevent and treat malaria may be re-deployed to support services experiencing increased pressures related to the COVID-19 pandemic. Additionally, all healthcare services must also manage the threat of health worker infection reducing the workforce capacity.[5] The unprecedented demand for personal protective equipment (PPE) has also proved challenging, and scenarios where PPE supplies are inadequate puts both the patient and healthcare providers at risk of infection and thus can interrupt the delivery of essential healthcare services.[12]
Disruption to supply chains: in addition to the effects on the healthcare workforce, there are also infrastructural and logistical challenges posed by the pandemic in maintaining essential malaria services. This is described in detail in the World Malaria Report 2020 [1] and refers to the impact of delays or reductions in the manufacturing of goods like insecticide treated nets - which are central to preventative programmes for malaria - due to factors including increasing costs for raw materials and restricted staffing in the factories producing these items. Furthermore, delays in transporting goods also occurred due to travel restrictions and lockdown measures which were necessary to try and control the transmission of COVID-19, but limited the movement of people and goods.[1] The WHO World Malaria Project’s guidance on Tailoring malaria interventions in the COVID-19 response again provides approaches to try and mitigate disruption to essential services, and emphasises the potential benefits of utilising and strengthening existing infrastructure for infectious diseases programmes to jointly address COVID-19 alongside the pre-existing disease burden.
Redirecting (repurposing) antimalarial medications for treatment of COVID-19: the antimalarial hydroxychloroquine (a derivative of chloroquine) has not been demonstrated to be beneficial against COVID-19 in hospitalised patients in the large-scale clinical trials, WHO Solidarity (arm-discontinued for futility) [13] and RECOVERY [14]. Emerging resistance has restricted the use of hydroxychloroquine as an antimalarial in recent years, although it is still an important therapeutic option particularly against plasmodium vivax.[1] Some authors highlight the risk that widespread use in the management of COVID-19 (especially if not clinically proven to be beneficial) will exacerbate selection of chloroquine-resistant parasites.[10] Furthermore, the World Malaria Report 2020 states that when sales of the active pharmaceutical compound (4,7-dichloroquinoline) peaked earlier this year following suggestion of therapeutic benefit for chloroquine and derivatives in COVID-19 infection, the supply of other antimalarial medication (such as piperaquine and amodiaquine) which also depend on this active compound was constrained.[1] Of note, the WHO highlight that further evaluation of hydroxychloroquine in non-hospitalised patients with COVID-19, or as a pre- or post-exposure prophylaxis, may demonstrate different results to the aforementioned trials which focus on in-hospital mortality from SARS-CoV-2 infection.[11]
Focussing research and development for rapid diagnostic tests on COVID-19: in the early stages of the pandemic, there was an urgent need to develop rapid diagnostic tests (RDTs) for SARS-CoV-2.[1, 10] This led to manufacturers diverting capacity towards the production of COVID-19 immunoassays, with the potential risk of a shortfall of RDTs for malaria. The malaria cross-partner task force have been working to try and ensure there is not a devastating shortage of malaria RDTs during the pandemic, and this has been discussed in greater detail within section 10 of the World Malaria Report 2020.[1]
Conclusion
The World Malaria Report 2020 highlights that progress in reducing morbidity and mortality from malaria has plateaued over the past four years, and the WHO has therefore called for reinvigorated action from the global community to address this.[1] The COVID-19 pandemic poses an additional challenge in achieving the goals set out in the ‘Global Technical Strategy for Malaria 2016–2030’, and it is essential that in addressing the pandemic, other high burden diseases such as malaria are not forgotten.[2, 5, 9, 15] Children, in particular, are likely to be disproportionately affected by disruptions to essential malaria services during the COVID-19 pandemic.[15]
As highlighted in the World Malaria Report 2020, integrating the existing management infrastructure for infectious diseases with measures for addressing COVID-19, combined with efforts to strengthen community healthcare systems, is likely to be an essential approach.[1] Furthermore, clear and consistent communication in public health messages which are adapted for malaria endemic settings is important to avoid conflicting advice that could risk people with fever delaying seeking treatment and result in untreated cases of malaria.[1, 11] Although this article has focussed on the impact of COVID-19 on malaria, the challenge of maintaining essential services for both communicable and non-communicable disease during a global pandemic has common themes which require a concerted global response to overcome.
Useful Resources:
WHO: World Malaria Report 2020
WHO (Guidance): Tailoring malaria interventions in the COVID-19 response
WHO: Coronavirus disease (COVID-19) and Malaria - Q&A
WHO: Malaria and COVID-19: country perspectives (webinar)
Continue the Discussion:
Join the COVID-19 discussion groups for healthcare professionals on MedShr:




References:
[1] World Health Organization. World malaria report 2020: 20 years of global progress & challenges. Geneva: World Health Organization; 2020 Nov 30. Licence: CC BY-NC-SA 3.0 IGO. Available at: www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2020
[2] Walker PGT, Whittaker C, Watson OJ, Baguelin M, Winskill P, Hamlet A, Djafaara BA, Cucunubá Z, Olivera Mesa D, Green W, Thompson H, Nayagam S, Ainslie KEC, Bhatia S, Bhatt S, Boonyasiri A, Boyd O, Brazeau NF, Cattarino L, Cuomo-Dannenburg G, Dighe A, Donnelly CA, Dorigatti I, van Elsland SL, FitzJohn R, Fu H, Gaythorpe KAM, Geidelberg L, Grassly N, Haw D, Hayes S, Hinsley W, Imai N, Jorgensen D, Knock E, Laydon D, Mishra S, Nedjati-Gilani G, Okell LC, Unwin HJ, Verity R, Vollmer M, Walters CE, Wang H, Wang Y, Xi X, Lalloo DG, Ferguson NM, Ghani AC. The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries. Science. 2020 Jul 24;369(6502):413-422. doi: 10.1126/science.abc0035. Epub 2020 Jun 12. PMID: 32532802; PMCID: PMC7292504.
[3] Wang J, Xu C, Wong YK, He Y, Adegnika AA, Kremsner PG, Agnandji ST, Sall AA, Liang Z, Qiu C, Liao FL, Jiang T, Krishna S, Tu Y. Preparedness is essential for malaria-endemic regions during the COVID-19 pandemic. Lancet. 2020 Apr 4;395(10230):1094-1096. doi: 10.1016/S0140-6736(20)30561-4. Epub 2020 Mar 17. PMID: 32192582; PMCID: PMC7158917.
[4] World Health Organization. The potential impact of health service disruptions on the burden of malaria: a modelling analysis for countries in sub-Saharan Africa. Geneva: World Health Organization. 2020. Available at: https://apps.who.int/iris/handle/10665/331845. License: CC BY-NC-SA 3.0 IGO
[5] World Health Organization. Tailoring malaria interventions in the COVID-19 response. Geneva: World Health Organization. 2020 Apr 9. Licence: CC BY-NC-SA 3.0 IGO. Available at: https://www.who.int/publications/m/item/tailoring-malaria-interventions-in-the-covid-19-response
[6] Plucinski MM, Guilavogui T, Sidikiba S, Diakité N, Diakité S, Dioubaté M, Bah I, Hennessee I, Butts JK, Halsey ES, McElroy PD, Kachur SP, Aboulhab J, James R, Keita M. Effect of the Ebola-virus-disease epidemic on malaria case management in Guinea, 2014: a cross-sectional survey of health facilities. Lancet Infect Dis. 2015 Sep;15(9):1017-1023. doi: 10.1016/S1473-3099(15)00061-4. Epub 2015 Jun 23. PMID: 26116183; PMCID: PMC4669675.
[7] Walker PG, White MT, Griffin JT, Reynolds A, Ferguson NM, Ghani AC. Malaria morbidity and mortality in Ebola-affected countries caused by decreased health-care capacity, and the potential effect of mitigation strategies: a modelling analysis. Lancet Infect Dis. 2015 Jul;15(7):825-32. doi: 10.1016/S1473-3099(15)70124-6. Epub 2015 Apr 23. PMID: 25921597; PMCID: PMC4824180.
[8] Bailey LC, Razzaghi H, Burrows EK, Bunnell HT, Camacho PEF, Christakis DA, Eckrich D, Kitzmiller M, Lin SM, Magnusen BC, Newland J, Pajor NM, Ranade D, Rao S, Sofela O, Zahner J, Bruno C, Forrest CB. Assessment of 135 794 Pediatric Patients Tested for Severe Acute Respiratory Syndrome Coronavirus 2 Across the United States. JAMA Pediatr. 2020 Nov 23:e205052. doi: 10.1001/jamapediatrics.2020.5052. Epub ahead of print. PMID: 33226415; PMCID: PMC7684518.
[9] Sherrard-Smith E, Hogan AB, Hamlet A, Watson OJ, Whittaker C, Winskill P, Ali F, Mohammad AB, Uhomoibhi P, Maikore I, Ogbulafor N, Nikau J, Kont MD, Challenger JD, Verity R, Lambert B, Cairns M, Rao B, Baguelin M, Whittles LK, Lees JA, Bhatia S, Knock ES, Okell L, Slater HC, Ghani AC, Walker PGT, Okoko OO, Churcher TS. The potential public health consequences of COVID-19 on malaria in Africa. Nat Med. 2020 Sep;26(9):1411-1416. doi: 10.1038/s41591-020-1025-y. Epub 2020 Aug 7. PMID: 32770167.
[10] Aborode AT, David KB, Uwishema O, Nathaniel AL, Imisioluwa JO, Onigbinde SB, Farooq F. Fighting COVID-19 at the Expense of Malaria in Africa: The Consequences and Policy Options. Am J Trop Med Hyg. 2020 Nov 11. doi: 10.4269/ajtmh.20-1181. Epub ahead of print. PMID: 33205743.
[11] World Health Organization. Coronavirus disease (COVID-19): Malaria and COVID-19 [internet]. Published 2020 Aug 25. Available at: https://www.who.int/news-room/q-a-detail/coronavirus-disease-covid-19-malaria-and-covid-19
[12] Talisuna A, Yoti Z, Lee C, Frieden TR, Moeti MR. The urgent need for a global commitment to protect healthcare workers. BMJ Glob Health. 2020 Nov;5(11):e004077. doi: 10.1136/bmjgh-2020-004077. PMID: 33154103; PMCID: PMC7646325.
[13] WHO Solidarity Trial Consortium, Pan H, Peto R, Henao-Restrepo AM, et al. Repurposed Antiviral Drugs for Covid-19 - Interim WHO Solidarity Trial Results. N Engl J Med. 2020 Dec 2. doi: 10.1056/NEJMoa2023184. Epub ahead of print. PMID: 33264556.
[14] RECOVERY Collaborative Group, Horby P, Mafham M, Linsell L, et al. N Engl J Med. 2020 Nov 19;383(21):2030-2040. doi: 10.1056/NEJMoa2022926. Epub 2020 Oct 8. PMID: 33031652; PMCID: PMC7556338.
[15] Coker M, Folayan MO, Michelow IC, Oladokun RE, Torbunde N, Sam-Agudu NA. Things must not fall apart: the ripple effects of the COVID-19 pandemic on children in sub-Saharan Africa. Pediatr Res. 2020 Sep 24. doi: 10.1038/s41390-020-01174-y. Epub ahead of print. PMID: 32971527.
Article by Dr Ryan Broll, MedShr Open Editorial Team, Medical Education Fellow
Loading Author...
Sign in or Register to comment